An accessory soleus is an anatomical variant characterized by an additional distinct muscle encountered along with a normal soleus muscle. The accessory soleus muscle is an incidental finding (Prevalence: variable range from 0.7-10%, maybe bilateral). It may become symptomatic because it is a soft tissue mass that hinders a free dorsal flexion of the foot. Besides, it may cause compression or displacement of the tibial nerve. The patient reported exercise-related pain in the (posterior) ankle, most likely due to changed biomechanics of the ankle, probably in combination with inadequate blood supply.
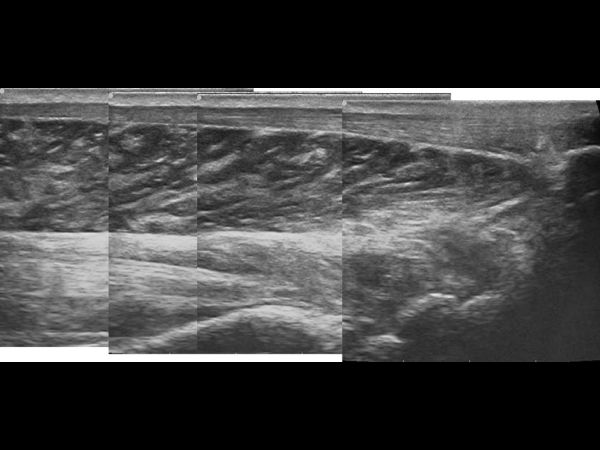
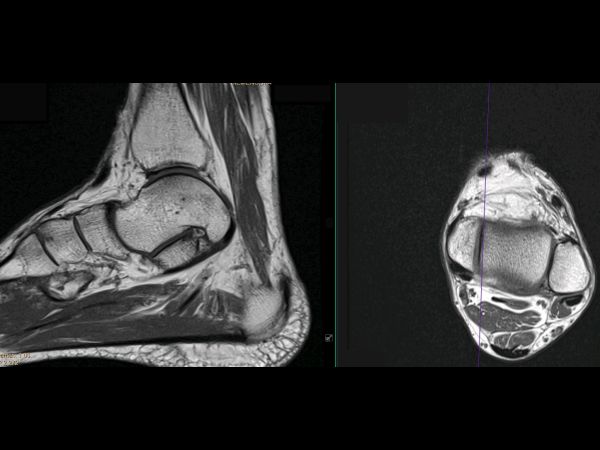
On plain radiography, accessory soleus may cause obliteration of Kager’s fat pad, but they are rarely diagnostic because of its low soft-tissue contrast. On ultrasound (US), the echotexture of accessory soleus is identical to other muscles, but the movement excursions related to dorsiflexion and plantarflexion are limited, the contraction was possible and visible. The signal intensity of the accessory soleus muscle is similar to muscle on all MR pulse sequences. Therefore, because of the intrinsic contrast with the adjacent Kager’s fat body, accessory soleus is best identified on T1-weighted images without FS. Both US and MRI may be used to evaluate the mass effect on the adjacent structures. The origin of this accessory soleus is from the deep aponeurosis of the soleus muscle; its insertion is a type 4 at the medial aspect of the os calcaneus as a direct muscular insertion. On examination, the patient presented the posteromedial mass of the ankle, which became stiff and tense in standing or tiptoe position and exercise-related pain during sports (posterior impingement syndrome). Differential diagnosis: Low myotendinous junction of the Flexor Hallucis Longus Muscle distal to the level of the posterior talocrural joint.
Pain most likely caused by an accessory soleus muscle, impinging the talocrural joint and becoming tens in a 90-degree standing position. There were no neurologic components in the clinical assessment, and the physical examination, so compression of the tibial nerve was excluded. In walking the patient presented a premature heel lift with the potential to develop metatarsalgia. Due to the changes in biomechanics, the ankle joint became painful, and we have called this ‘posterior impingement syndrome.’


Robert is a specialist in foot and ankle sonography. He studied Podiatry and in 2004, Robert founded Podiatry Care Netherlands. Since 2007 he specialized in rheumatism and ultrasonography.
More Cases from Robert Wonink


